| home | research | people | alzheimer's disease | get involved! |
It is thought that
dual-tasking, the
ability to do
two things at once, is a product of the brain’s ability to
coordinate. We
understand this dual-task coordination to be part of ‘working
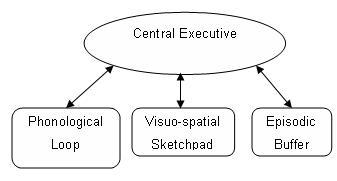
memory’. In 1974, scientists Alan Baddeley and Graham Hitch
proposed that short-term memory
should be thought of as ‘working memory’, which can
store
and maintain a
certain amount of information temporarily. Information may be
phonological
(sounds/language) or visuo-spatial (vision/space). Phonological
information,
such as a friend’s telephone number, is handled by the
‘phonological loop’ and
visuo-spatial information, such as the route you would plan to take to
go to
your friend’s house, is handled by the
‘visuo-spatial
sketchpad’.
Baddeley’s (2000) Model
of Working Memory
what
happens to dual-tasking
ability in alzheimer’s disease?
In
1986, Baddeley, Logie, Bressi, Della Sala and Spinnler reported that
people
with Alzheimer’s disease (AD) demonstrate a selective
impairment in
dual-tasking. They based their conclusions on studies comparing people
with AD
with healthy young and older adults, performing two tasks at once: a
tracking
task as well as an articulatory suppression, simple reaction time to
tone or
auditory digit span task. They found that when tracking was paired with
simple
reaction time or digit span task (but not articulatory suppression),
the people
with AD performed dramatically lower than the healthy young or older
adults.
This effect remained even when the difficulty of the tracking task, and
the
length of digit span were adjusted, so as to equate performance across
the
three groups when the tasks were performed alone. The group
hypothesised that
this effect was not seen when the tracking task was paired with the
articulatory suppression task because it was not sufficiently demanding
to
require the participant to dual-task.
These experiments and findings suggest that that AD features a specific impairment in the central executive. Further research has found that dual-task performance correlates with the presence of behavioural problems (Baddeley, Della Sala, Papagno & Spinnler, 1997b) and difficulties in people with AD performing everyday tasks that require dual-tasking, such as keeping track of conversations (Alberoni, Baddeley, Della Sala, Logie & Spinnler, 1992) or talking while walking (Cocchini, Della Sala, Logie, Pagani, Sacco & Spinnler, 2004).
how can this be developed into a
clinical tool?
Currently, assessments
of memory functioning are
thought to be the most useful tests to detect AD. These tests are very
sensitive to AD, but unfortunately as memory difficulties can be
present in
many other types of disorders and even in normal ageing, these tests
are not
specific to AD. This can lead to diagnostic uncertainty, worrying for
both
patient and significant others, or worse, incorrect diagnosis of AD.
These
tests, therefore, require further components to improve their
specificity.
references
| Alberoni, M., Baddeley, A., Della Sala, S., Logie, R. H. & Spinnler, H. (1992). Keeping track of a conversation: Impairments in Alzheimer's disease. International Journal of Geriatric Psychiatry, 7, 639-646. | |
| Baddeley,
A. D. & Hitch, G. J. (1974). Working memory. In G. H. Bower
(Ed.), The
psychology of learning and motivation
(Vol. 8; pp 47 - 89). |
|
| Baddeley, A. D, Bressi, S., Della Sala, S., Logie, R. H. & Spinnler, H. (1991). The decline in working memory in Alzheimer’s disease: A longitudinal study. Brain, 114, 2521 – 2542. | |
| Baddeley, A., Della Sala, S.,
Gray, C., Papagno, C.,
& Spinnler, H. (1997a). Testing central executive functioning
with a
pencil-and-paper test. In P. Rabbitt (Ed.), Methodology
of frontal and executive function (pp. 61 -
80). Hove: Psychology Press. |
|
| Baddeley, A., Della Sala, S., Papagno, C., & Spinnler, H. (1997b). Dual-task performance in dysexecutive and nondysexecutive patients with a frontal lesion. Neuropsychology, 11, 187-194. | |
| Baddeley, A. D., Logie, R.,
Bressi, S., Della Sala, S., & Spinnler, H. (1986). Dementia and
working memory. Quarterly Journal of Experimental
Psychology, 38A, 603-618. |
|
| Clare, L., Woods, B.,
Moniz-Cook, E., Orrell, M. & Spector, A. (2005). Cognitive
rehabilitation interventions targeting
memory functioning in
early-stage Alzheimer's disease and vascular dementia.
Systematic review.
Cochrane Library. |
|
| Cocchini, G, Della Sala, S., Logie, R. H., Pagani, R., Sacco, L. & Spinnler, H. (2004). Dual task effects of walking while talking in alkzheimer disease. Revue Neurologique, 160, 74-80. | |
| Della Sala, S., Baddeley, A., Papagno, C. & Spinnler, H. (1995). Dual task paradigm: A means to examine the central executive. In J. Grafman, K. J. Holyoak, F. Boller (Eds.). Structure and functions of the human prefrontal cortex. Vol. 769. New York: Annals of the New York Academy of Sciences, pp. 161-171. | |
| Giacobini,
E. (2000).
Cholinesterase inhibitors stabilize Alzheimer’s disease. Annals of the |
|
| Logie, R.H., Cocchini, G., Della Sala, S. & Baddeley, A.D. (2004). Is there a specific executive capacity for dual task co-ordination? Evidence from Alzheimer’s Disease. Neuropsychology 18, 504-513. |